Managing diabetes is not just about lowering one number. It is also about reducing the risk of complications before they become harder to manage.
Blood glucose is still central to diabetes care, but diabetes management is broader than day-to-day glucose alone. Over time, diabetes can affect the kidneys, heart and blood vessels, eyes, and nerves. That is why good diabetes care usually includes more than glucose checks. It involves a broader monitoring plan that helps people and their healthcare teams track current glycemic status, longer-term trends, and early signs of complications. NIDDK explains that high blood glucose over time can contribute to heart disease, kidney disease, nerve damage, and eye disease. (NIDDK). Because these complications often develop gradually, the ADA recommends routinely monitoring key health indicators such as A1C, cholesterol, kidney function, blood pressure, along with regular eye exams, to identify potential issues early. (ADA)
Why diabetes care involves more than blood glucose alone
That is why diabetes care is not only about asking, “What is my glucose today?” It is also about asking, “How well am I managing my diabetes overall?” The answer lies in a broader picture of health—one that includes glycemic control, kidney health, cardiovascular risk factors, and regular screening for diabetes-related complications. NIDDK’s “ABCs” framework also reinforces this broader view: A stands for A1C, B for blood pressure, and C for cholesterol, because all three matter for long-term outcomes. (NIDDK)
A useful way to think about diabetes monitoring is this: some checks help you manage what is happening now, while others help you understand what may be building over time. Blood glucose is closer to the first category. A1C, kidney tests, blood pressure, lipids, and screening exams help address the second. (NIDDK)
PART 1. What to monitor in diabetes care
A. Glycemic Monitoring
Blood glucose is the amount of glucose circulating in the bloodstream at a given moment. It reflects a person’s current glucose status and helps show how meals, exercise, medication, illness, and stress affect glucose throughout the day.
In general, a fasting blood glucose level below 100 mg/dL is considered normal, 100 to 125 mg/dL indicates prediabetes, and 126 mg/dL or higher may indicate diabetes.
A1C is a measure of the percentage of hemoglobin in red blood cells that has glucose attached to it. Because red blood cells live for about 2 to 3 months, A1C reflects a person’s average blood glucose level over the past 2 to 3 months rather than just a single moment in time.
NIDDK notes that an A1c below 5.7% is generally considered normal, 5.7% to 6.4% indicates prediabetes, and 6.5% or higher indicates diabetes. (NIDDK)
| Category | A1C | Fasting Blood Glucose |
|---|---|---|
| Normal | Below 5.7% | Below 100 mg/dL |
| Prediabetes | 5.7–6.4% | 100–125 mg/dL |
| Diabetes | 6.5% or higher | 126 mg/dL or higher |
B. Kidney health monitoring
eGFR stands for estimated glomerular filtration rate. It is a calculation based on a blood creatinine test and is used to estimate how well the kidneys are filtering blood. In general, an eGFR of 90 or above is considered in the normal range, while an eGFR 60 may suggest reduced kidney function or chronic kidney disease.
UACR stands for urine albumin-to-creatinine ratio. It measures how much albumin is present in the urine relative to creatinine. Albumin is a protein that normally stays in the blood. When the kidneys are damaged, some of it can leak into the urine. In general, a UACR below 30 mg/g is considered normal, while that of 30mg/g or higher may indicate abnormal albumin leakage. (NIDDK).
| Test | Generally Considered Normal |
|---|---|
| eGFR | 90 or higher |
| UACR | Below 30 mg/g |
NIDDK identifies urine albumin and eGFR as the two key markers for chronic kidney disease.(NIDDK)
C. Cardiovascular and metabolic health monitoring
Readings below 120 mmHg for systolic pressure and below 80 mmHg for diastolic pressure are considered normal. “Elevated Blood Pressure” refers to systolic readings of 120–129 mmHg with diastolic readings below 80 mmHg. “Stage 1 Hypertension” refers to systolic readings of 130–139 mmHg or diastolic readings of 80–89 mmHg, while “Stage 2 Hypertension” refers to systolic readings of 140 mmHg or higher or diastolic readings of 90 mmHg or higher.
| Category | Blood Pressure |
|---|---|
| Normal | <120 and <80 mmHg |
| Elevated Blood Pressure | 120–129 and <80 mmHg |
| Stage 1 Hypertension | 130–139 or 80–89 mmHg |
| Stage 2 Hypertension | ≥140 or ≥90 mmHg |
Cholesterol and triglycerides are commonly measured together as part of a lipid panel, which helps assess cardiovascular and metabolic risk. cholesterol, HDL cholesterol, and triglycerides. A standard lipid panel typically includes total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides, each providing different information about heart and metabolic health.
Total cholesterol measures the total amount of cholesterol in the blood, including LDL cholesterol, HDL cholesterol, and other cholesterol-containing particles. While it provides a general overview of cholesterol levels, healthcare providers often look at LDL, HDL, and triglycerides separately to better assess cardiovascular risk.
LDL cholesterol stands for low-density lipoprotein cholesterol. It carries cholesterol from the liver to the body’s tissues. When LDL levels are too high, cholesterol can build up in artery walls, which is why LDL is often called “bad” cholesterol. In general, an LDL level below 100 mg/dL is considered optimal, 100 – 129 mg/dL is near or above optimal, 130 – 159 mg/dL is borderline high, 160 – 189 mg/dL is high, and 190 mg/dL or higher is very high.
HDL cholesterol stands for high-density lipoprotein cholesterol. It helps remove excess cholesterol from the bloodstream and carries it back to the liver for disposal. Because of that role, HDL is often called “good” cholesterol. In general, an HDL level below 40 mg/dL in men or below 50 mg/dL in women is considered low, while 60 mg/dL or higher is generally considered protective.
Triglycerides are a type of fat that stores excess energy from food. Elevated triglycerides levels may indicate metabolic dysfunction and are associated with increased cardiovascular risk, especially when they occur together with low HDL or high LDL cholesterol. In general, a triglyceride levels below 150 mg/dL is considered normal, 150 – 199 mg/dL is borderline high, 200 – 499 mg/dL is high, and 500 mg/dL or higher is very high.
| Lipid Test | Optimal / Normal | Borderline | High | Very High |
|---|---|---|---|---|
| LDL Cholesterol | Below 100 mg/dL | 130–159 mg/dL | 160–189 mg/dL | ≥190 mg/dL |
| Triglycerides | Below 150 mg/dL | 150–199 mg/dL | 200–499 mg/dL | ≥500 mg/dL |
| HDL Cholesterol | Interpretation |
|---|---|
| Below 40 mg/dL (men) | Low |
| Below 50 mg/dL (women) | Low |
| 60 mg/dL or higher | Generally considered protective |
ADA includes cholesterol monitoring among routine checks for people with diabetes because cardiovascular disease remains such an important part of diabetes management. (NIDDK)
D. Diabetes complication screening
While the biomarkers discussed above provide important information about diabetes management and overall health, they do not directly detect every diabetes-related complication. Some complications can develop gradually and remain unnoticed until significant damage has already occurred. For that reason, routine complication screening is an important part of diabetes care. Among the most commonly recommended screenings are eye exams and foot exams, as the eyes and feet are particularly vulnerable to diabetes-related damage affecting small blood vessels and nerves. These exams can help identify early signs of complications before they progress to vision loss, foot ulcers, infection, or amputation. (CDC)
Eye exams are used to screen for diabetic retinopathy and other diabetes-related eye complications. High blood glucose over time can damage the small blood vessels in the retina, sometimes before symptoms become noticeable. CDC estimated that in 2021, about 9.6 million people in United States were living with diabetic retinopathy, and among people with diabetes, the prevalence ranged from 13.0% in younger age groups to 28.4% in adults ages 65 to 79. That is why regular eye exams are important: they help identify retinal changes early, before vision loss becomes more likely. (CDC)
Foot exams assess nerve function, circulation, skin health, and ulcer risk. Diabetes can damage nerves and blood vessels, which may lead to reduced sensation, poor wound healing, and increased risk of infection or amputation if problems go unnoticed. CDC notes that about half of all people with diabetes have some kind of nerve damage, most often affecting the feet and legs. CDC also reports that about 12% of people with diabetes develop diabetic foot ulcers during their lifetime. Regular foot exams help detect early signs of neuropathy and circulation problems before they progress to ulcers, infection, or lower-extremity amputation. (CDC, CDC)
What each biomarker can tell you
Each biomarker tells a different part of the diabetes story. Some markers help explain what is happening right now, while others help show what has been happening over time – or whether diabetes may already be affecting organs such as the kidneys, blood vessels, eyes or nerves. That is why looking at one number alone is rarely enough.
Blood Glucose
Blood glucose is the most immediate marker in diabetes care. It helps show what is happening in real time.
When blood glucose is too high, it may suggest that insulin is not sufficient, is not working effectively enough, or that recent food intake, illness, stress, or medication changes are pushing glucose out of range. A high reading does not just reflect “extra sugar”. It may signal that the body is not using glucose properly and that tissues are being exposed to higher-than-normal glucose stress.
When blood glucose is too low, the concern is not just “a low number.” It may mean the body does not have enough readily available glucose to function normally, which can lead to shakiness, sweating, confusion, weakness, or even severe hypoglycemia. Severe hypoglycemia can become a medical emergency if not treated promptly. For people taking insulin or certain diabetes medications, blood glucose monitoring is important not only for tracking glucose levels, but also for detecting low glucose early. That matters because hypoglycemia can develop quickly and may lead to symptoms such as shakiness, sweating, confusion, weakness, or, in more severe cases, loss of consciousness or a medical emergency.
In practical terms, blood glucose helps answer the question:
What is happening right now, and do I need to respond today?
A1C
A1C tells a different story. It is not about what is happening right now – It is about what has been happening consistently over time.
That distinction matters because many diabetes complications do not develop from one isolated high reading. They develop when blood glucose remains elevated often enough, and long enough, to gradually damage blood vessels and organs. A higher A1C may therefore suggest that glucose has been running high over the past 2 to 3 months, even if some individual readings looked acceptable on certain days.
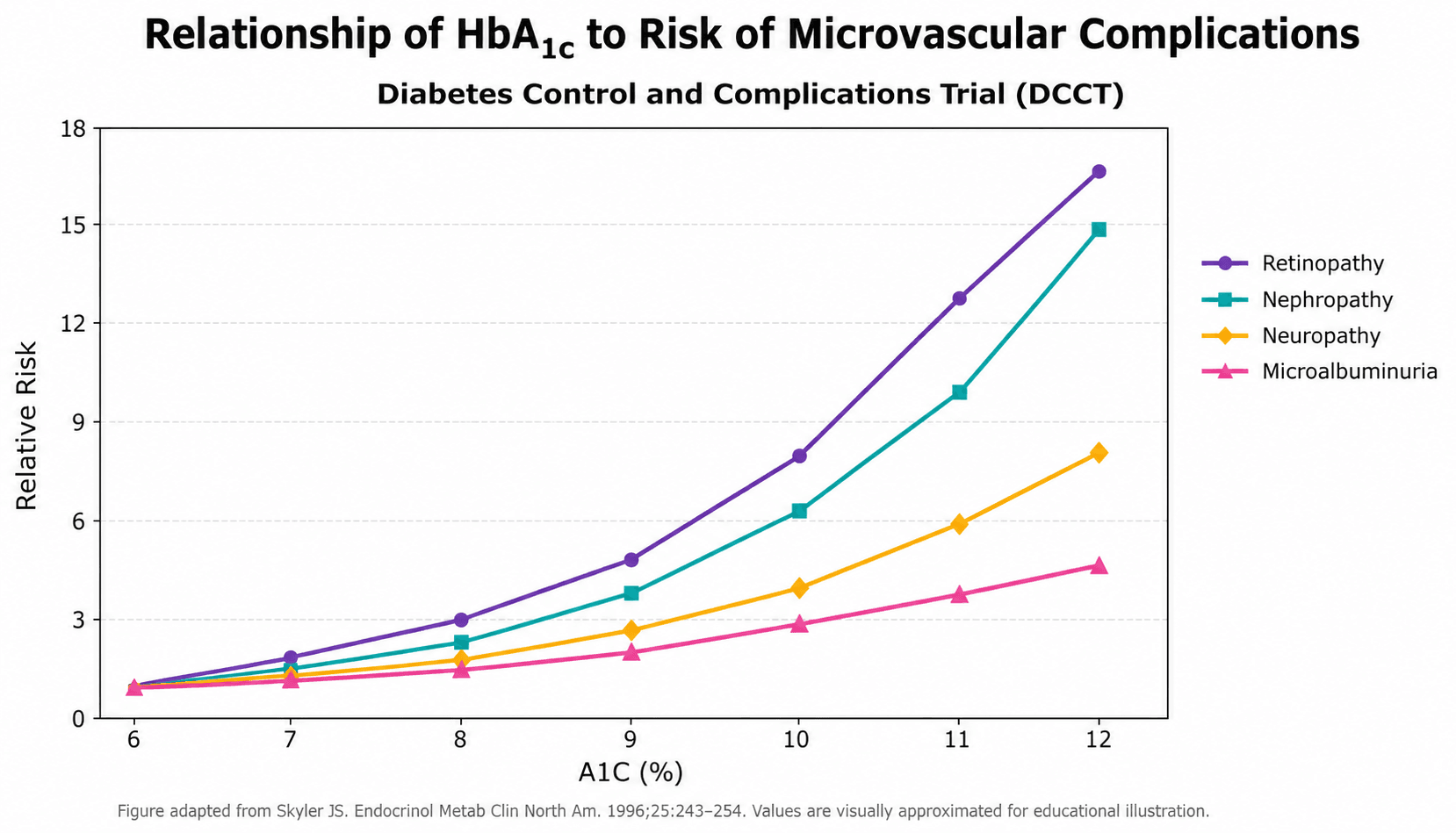
This is why A1C is often treated as more than just a monitoring number. It is also one of the clearest markers of long-term complication risk. The DCCT (Diabetes Control and Complication Trial) study is one of the strongest examples of this. As shown below, the risk of diabetes-related microvascular complications—including retinopathy, nephropathy, neuropathy, and microalbuminuria—increases progressively as A1C rises.
That makes A1C more than a summary of the past few months. It is one of the most useful ways to understand why long-term glucose control matters.
A simple way to explain the difference is this:
- Blood glucose shows a snapshot of how your body is responding to glucose right now.
- A1C shows a longer-term view of how well diabetes is being managed.
eGFR and UACR
These two kidney markers are often interpreted together because they do not tell the same story.
A lower eGFR may suggest that the kidneys are losing filtering capacity over time. In practical terms, it helps show whether kidney function may be declining and whether chronic kidney disease could be progressing. That is what makes eGFR especially useful for understanding overall kidney function.
An elevated UACR, by contrast, may be an early sign that the kidneys are becoming damaged, even before overall kidney function begins to decline. In other words, UACR can sometimes become abnormal earlier in the disease process, while eGFR may remain relatively preserved at first. That is why UACR is especially valuable for identifying early kidney injury, while eGFR is more useful for understanding how well the kidneys are functioning overall.
That difference matters because these two tests answer different clinical questions. A patient may have an elevated UACR while eGFR is still in a relatively preserved range, suggesting that kidney damage may already be starting even though overall filtration has not yet fallen significantly. On the other hand, a lower eGFR may suggest that kidney function is already declining, which may indicate more advanced or progressing disease.
A simple way to think about it is this:
- eGFR may show declining kidney function
- UACR may show early kidney damage
Blood pressure
Blood pressure helps show how much strain the vascular system may be under over time. When it remains elevated, it may suggest greater stress on the blood vessels and a higher long-term risk of complications such as heart disease, stroke, and kidney damage. This is particularly important in diabetes because high blood pressure is common, affecting 6 out of 10 of people who have diabetes(CDC). Together, diabetes and hypertension can accelerate damage to blood vessels throughout the body, making blood pressure one of the most important markers of long-term cardiovascular risk.
Cholesterol and triglycerides
People often think of diabetes as a condition that only affects blood glucose. However, diabetes is fundamentally a disorder involving insulin, the hormone that helps regulate how the body uses and stores energy. Insulin helps regulate not only glucose, but also the way the body stores, releases, and transports fats. When insulin action becomes impaired, changes in cholesterol and triglyceride levels often occur alongside changes in blood glucose. For that reason, lipid markers are routinely monitored in diabetes care to provide a broader picture of metabolic and cardiovascular health.
Rather than focusing on a single number, healthcare providers often look at LDL cholesterol, HDL cholesterol, and triglycerides together. The overall pattern can provide insight into cardiovascular health, insulin resistance, and how diabetes may be affecting the body beyond glucose control alone.
In practical terms, lipid markers help answer the question:
What do my cholesterol and triglyceride levels reveal about my long-term cardiovascular and metabolic health?
PART 2. How often should these checks be done?
Many diabetes- related changes are silent. That means a person can feel well while important changes are already happening in blood vessels, kidneys, eyes, nerves, or circulation. If people with diabetes wait until they can feel that something is wrong, it may already be harder to prevent or manage complications. That is why these biomarkers and screening tests matter: they can help identify risk earlier, track changes over time, and catch complications before they become more serious. Knowing the usual timing of these checks is part of putting diabetes prevention into practice. (CDC)
The exact schedule still depends on the individual, but some general patterns are commonly used in diabetes care. (ADA)
Blood glucose
A1C
Blood pressure
Cholesterol and triglycerides
eGFR and UACR
Eye exam
Complete foot exam
Summary Table
| Check | What It Helps Monitor | Common Timing | ADA / General Guidance |
|---|---|---|---|
| Blood glucose | Current glucose status, short-term glucose patterns, and immediate risk such as hypoglycemia or out-of-range glucose changes | Depends on treatment plan; often more frequent with insulin use, medication changes, or hypoglycemia risk | Blood glucose monitoring is individualized. People using insulin, people at higher risk for hypoglycemia, or people who recently changed treatment may need more frequent checks. |
| A1C | Assessment of treatment effectiveness, long-term risk of diabetes-related complications, and average blood glucose over the past 2 to 3 months | Often every 3 to 6 months | ADA: every 6 months if in goal range; every 3 months if medications changed or not at target. |
| Blood pressure | Vascular stress, cardiovascular risk, stroke risk, and kidney-related risk beyond glucose alone | Commonly checked at routine visits | Blood pressure is commonly checked at healthcare visits and may also be monitored at home between visits. Closer follow-up may be needed if blood pressure is elevated or treatment is changing. |
| LDL / HDL / Triglycerides | Cardiovascular and metabolic risk | Periodically, depending on risk and treatment | Lipid testing is generally done periodically rather than constantly. Timing depends on age, cardiovascular risk, prior results, and whether lipid-lowering therapy is being used. |
| eGFR | Overall kidney function and whether kidney filtration may be declining over time | Often at least yearly | Kidney-related testing is typically done at least yearly in people with diabetes, with more frequent monitoring if kidney risk is higher or clinical status changes. |
| UACR | Early kidney damage, including albumin leakage that may appear before kidney function declines | Often at least yearly | ADA: target UACR < 30 mg/g urine creatinine; CDC lists kidney tests yearly. |
| Eye exam | Diabetic retinopathy and other diabetes-related eye complications before vision symptoms become obvious | Often yearly | CDC: dilated eye exam every year, more often if diabetes-related eye problems are present. ADA says timing depends on diabetes type and duration. |
| Complete foot exam | Neuropathy, reduced circulation, skin breakdown, ulcer risk, and other foot-related complications | At least yearly | CDC: complete foot check every year, more often if there has been diabetes-related foot trouble. |
Why A1C Remains Central to Diabetes Care
Among the many tests used in diabetes care, A1C occupies a unique position. It is one of the most widely used and clinically important indicators of how well diabetes is being managed over time. While A1C does not directly measure blood pressure, kidney function, cholesterol levels, or diabetes-related complications, it reflects long-term glucose exposure—a key factor linked to many of these outcomes. As a result, A1C has become one of the most important biomarkers for assessing treatment effectiveness and estimating long-term complication risk.
What good diabetes monitoring looks like in practice
A strong diabetes monitoring plan is not just a list of tests. It is a system in which different checks serve different purposes.
Some tests, such as blood glucose, help guide day-to-day decisions. Others, such as A1C, provide a longer-term view of diabetes management. Kidney tests, blood pressure, and lipid markers help assess how diabetes may be affecting overall metabolic, cardiovascular, and kidney health. Screening exams, including eye exams and foot exams, help identify complications that may develop silently before symptoms appear.
No single test can provide a complete picture. Each check answers a different question, and together they help build a more comprehensive understanding of current health, long-term risk, and potential complications.
Questions to ask your healthcare provider
It may help to ask:
- Which diabetes checks matter most for me right now?
- How often should I check my blood glucose and A1C?
- What do my recent A1C results suggest about my overall diabetes management?
- Are my blood pressure, cholesterol, and kidney markers within the target range?
- Based on my health history, how often should I have eye exams and foot exams?
- Are there any diabetes-related complications that I should be screened for?
- Which numbers should I pay the closest attention to between visits?
- What can I do to improve my results before my next checkup?
These questions can help shift the conversation from “What is my number today?” to “What does my overall monitoring plan look like?”
Frequently asked questions (FAQ)
If my blood glucose looks okay, does that mean my complication risk is low?
Not necessarily. Blood glucose is important, but complication risk is also shaped by longer-term glucose exposure, blood pressure, cholesterol, kidney health, and screening results. A reassuring glucose reading does not replace broader monitoring because diabetes-related complications can still develop gradually over time.
If my A1C is in range, do I still need kidney, eye, and foot checks?
Yes. A1C is important, but it does not replace kidney testing or complication screening. These checks address different parts of diabetes risk, including organ health and early signs of damage.
When should ketones be checked, and why are they not part of routine monitoring for everyone?
Ketone testing is not part of routine monitoring for every person with diabetes, but it becomes important when the risk of diabetic ketoacidosis, or DKA, is higher. CDC says ketones should be checked if a person with diabetes is sick, if blood glucose is 250 mg/dL or higher, or if symptoms of DKA are present. ADA also recommends checking ketones every 4 to 6 hours when you are feeling sick. DKA is most common in people with type 1 diabetes, but people with type 2 diabetes can also develop it. Warning signs include high blood glucose, high ketones, thirst or dry mouth, frequent urination, drowsiness, dry or flushed skin, nausea, vomiting, abdominal pain, difficulty breathing, fruity-smelling breath, and confusion. (CDC)
Can diabetes complications develop without symptoms?
Yes. Some complications, especially kidney disease, eye disease, and nerve-related problems, can develop gradually and without obvious symptoms. That is one reason routine monitoring and screening matter so much.
Can I rely on GMI alone to assess glucose control?
GMI is an estimate based on CGM mean glucose, while HbA1c is a laboratory measurement of glycated hemoglobin. Because these two values do not always match closely enough in individual patients, GMI should not be used alone to assess glucose control on its own.
A better approach is to interpret glucose control using more than one measure. Laboratory HbA1c, CGM mean glucose, and Time in Range (TIR) each provide different information, and looking at them together can give a more complete picture than relying on GMI alone.
In other words, GMI can be a helpful reference point, but it should not be treated as a replacement for laboratory HbA1c.
I was diagnosed recently. Which checks should I pay attention to first?
Blood glucose and A1C are usually central early on, but diabetes care should not stop there. Blood pressure, kidney tests, cholesterol, and baseline eye and foot assessments may also be important depending on the person’s overall risk profile and treatment plan.
Why are kidney tests so important in diabetes care?
Kidney tests are important because kidney disease is common in people with diabetes and often develops silently. CDC estimates that about 4 in 10 adults with diabetes have chronic kidney disease, and another CDC page states that approximately 1 in 3 adults with diabetes may have CKD. Diabetes is also the leading cause of kidney failure in the United States. eGFR helps assess kidney function, while UACR can detect early kidney damage before kidney function declines. Looking at both together gives a better picture than either one alone.
Why are LDL cholesterol and triglycerides important in diabetes care?
They help assess cardiovascular and metabolic risk. That matters because people with diabetes already face higher cardiovascular risk, and glucose control alone does not fully explain heart and vascular risk. LDL, HDL, and triglycerides help show whether broader cardiometabolic risk may still need attention even when glucose markers are being monitored closely.
Do all diabetes checks have to be done in a clinic?
No. Some diabetes-related checks can also be done at home, depending on the person’s care plan and the tools available. Blood glucose can be monitored with a meter or CGM, blood pressure can often be checked at home, and ketones can also be checked at home when needed. Some people may also choose to discuss at-home A1C testing with their healthcare provider. Other checks, such as many lab-based kidney or lipid tests and eye exams, still usually require clinic, lab, or specialist follow-up.
Can A1C only be checked in a clinic, or can it also be checked at home?
A1C is often checked in a clinic or laboratory, but for some people, at-home A1C testing may also play a useful role. It can help provide more visibility into longer-term glucose trends between routine visits, especially for people who want to better understand whether their overall diabetes management is moving in the right direction.
Final thought
Good diabetes care is not one-number management. It is about understanding:
- What to check
- Why They Matter
- How Often to Check
The better people understand the broader picture, the more meaningful and actionable each number becomes.
Good diabetes care means looking beyond a single number. Blood glucose, A1C, kidney markers, blood pressure, lipids, and complication screening each reveal a different part of the picture – and understanding them together can lead to earlier action and better long-term care.
No single number tells the whole story—but A1C remains one of the most important measures of long-term glucose management. Read More
Discover how at-home A1C testing can help you stay connected to your diabetes health between healthcare visits. Learn More